Zwei zeitgleich ablaufende neuroinflammatorische Prozesse tragen zur Akkumulation von Behinderung in der MS bei1-5
Immer mehr Anzeichen deuten darauf hin, dass akute und schwelende Neuroinflammation die Behinderungsakkumulation von Beginn der Erkrankung an vorantreiben – wobei letztere einen größeren Anteil zu haben scheint1-5
Verstehen, wie die Progression erfolgt
Anschauen, wie akute und schwelende Neuroinflammation die Behinderungsakkumulation beeinflussen

Akute Neuroinflammation – teilweise vorangetrieben durch aktivierte B-Zellen und T-Zellen aus der Peripherie – führt zu Schüben, akuten Läsionen und schubabhängiger Verschlechterung (RAW).1,3,6

Schwelende Neuroinflammation – im Wesentlichen vorangetrieben durch krankheitsassoziierte Mikrogila im ZNS – manifestiert sich klinisch als schubunabhängige Aktivität (PIRA).1,3,6
Die Pathophysiologie akuter und schwelender Neuroinflammation7,8
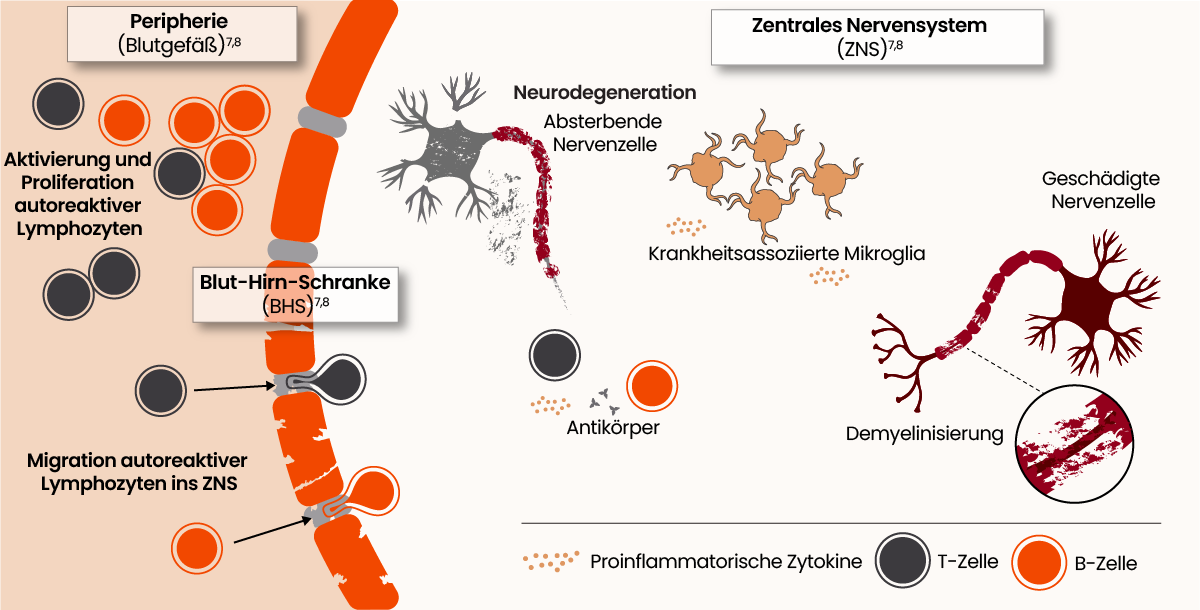
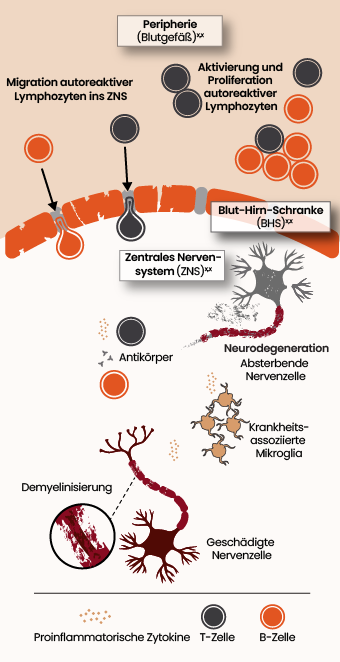
In der Vergangenheit wurde MS als eine durch adaptive Immunzellen aus der Peripherie, wie B-Zellen und T-Zellen, ausgelöste Erkrankung betrachtet. Inzwischen wächst das Verständnis für die entscheidende Rolle, die angeborene, ZNS-spezifische Immunzellen, vor allem Mikroglia, in der Behinderungsakkumulation spielen könnten.9
Mikroglia sind Hauptakteure der schwelenden Neuroinflammation im ZNS, die zu Behinderungsakkumulation führt9-12
Mikroglia werden in SPMS hochreguliert und spielen eine wesentliche Rolle bei der Behinderungsakkumulation.13,14
Eisenhaltige Mikroglia setzen sich am Rand von paramagnetischen Rand-Läsionen* (PRLs) ab und sind assoziiert mit einer erhöhten Behinderung sowohl in der RRMS als auch der SPMS in Verbindung gebracht.15
Durch Mikroglia ausgelöster Verlust von Synapsen ist assoziiert dem Verlust kognitiver Fähigkeiten.16-18
*PRLs gehören zu den chronischen aktiven Läsionen (CAL)
Die Bruton-Tyrosinkinase (BTK) ist ein vielversprechender neuer Ansatz der Forschung6,19
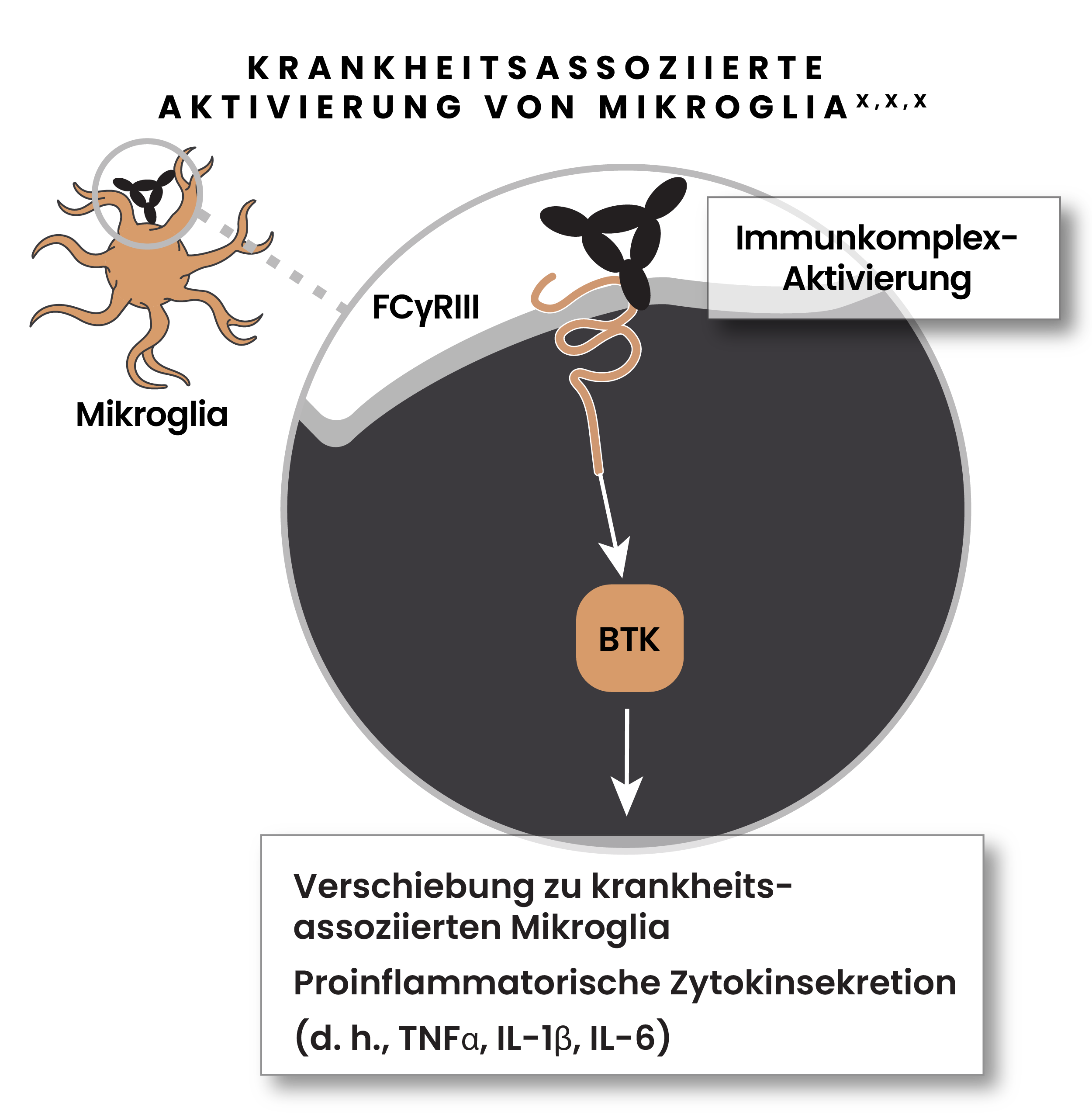
BTK ist wichtig für die Aktivierung von B-Zellen und Mikrogila bei der MS.6,19
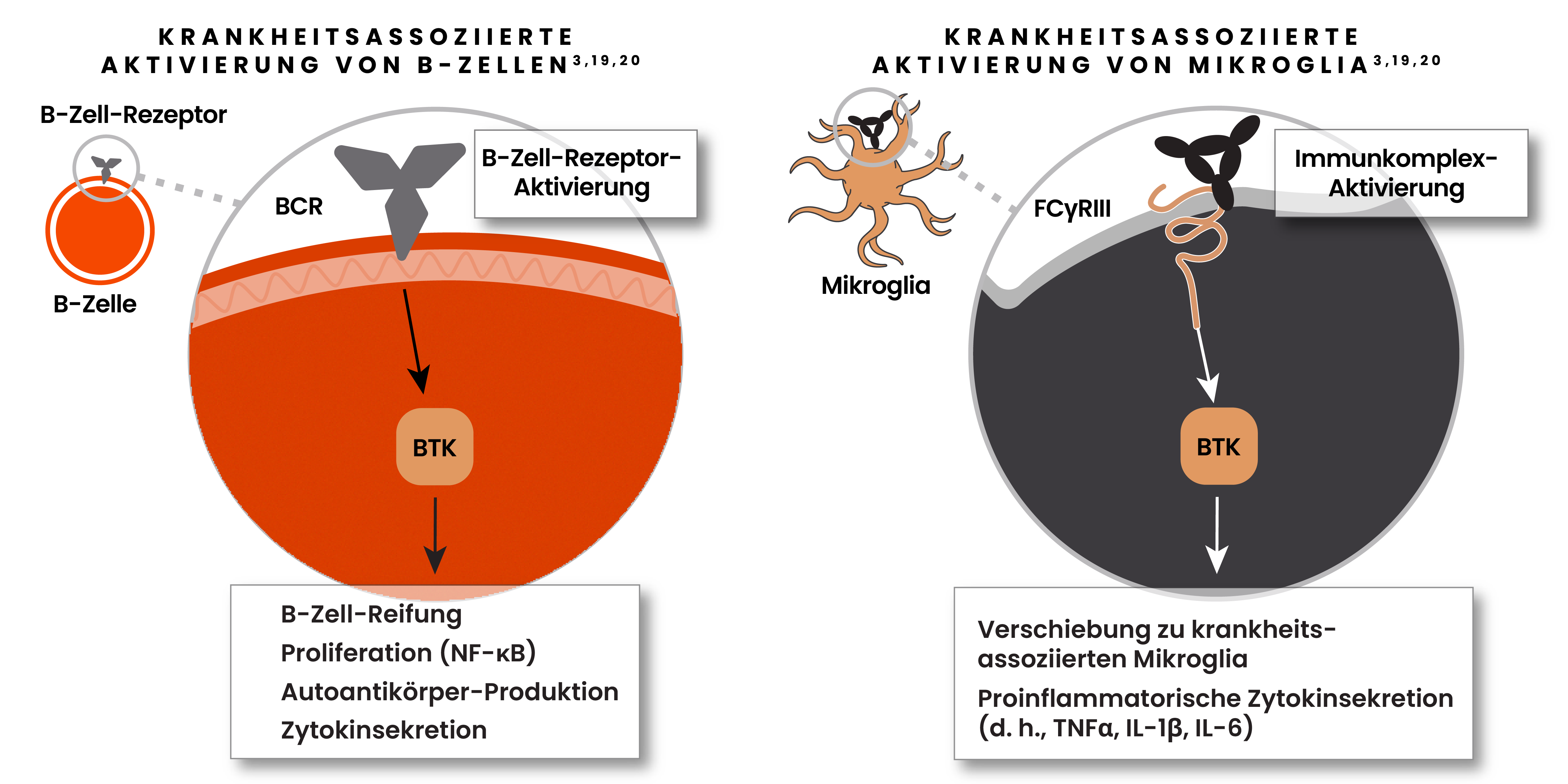
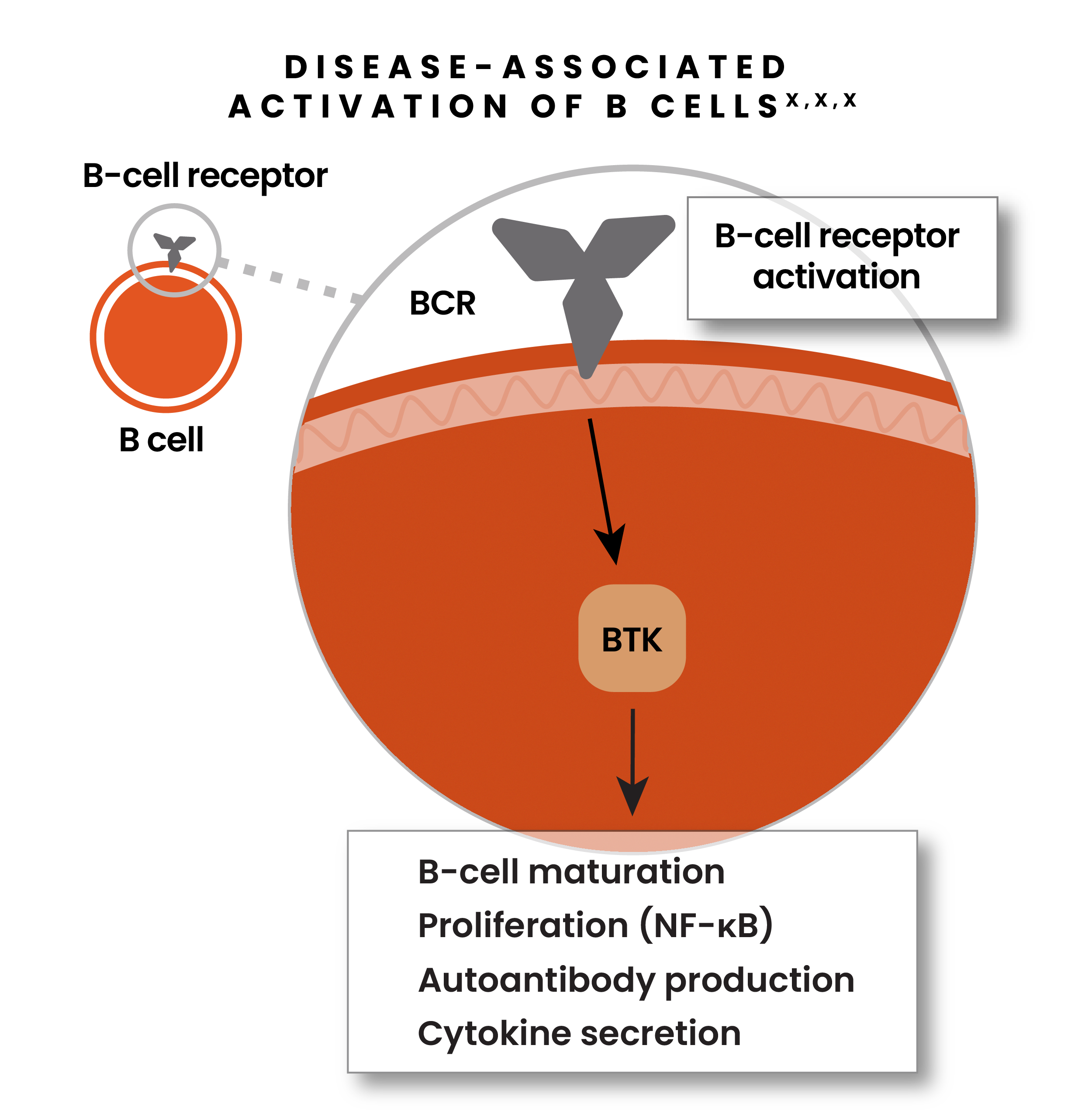
- BTK fördert die Proliferation, Antikörperproduktion und Zytokinsekretion in B-Zellen6,19
- Einmal aktiviert, kann die BTK einen Shift der Mikroglia aus ihrem homöostatischen in ihren krankheitsassoziierten Zustand auslösen6,19
- BTK ist in Mikroglia innerhalb des Läsionsgewebes bei SPMS-Patient*innen stark ausgeprägt6,19
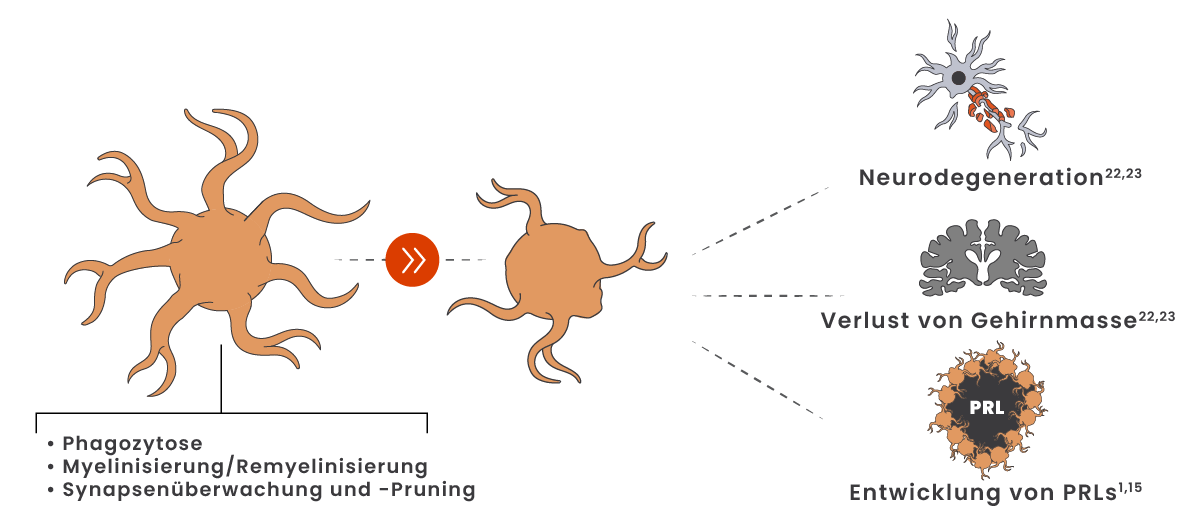
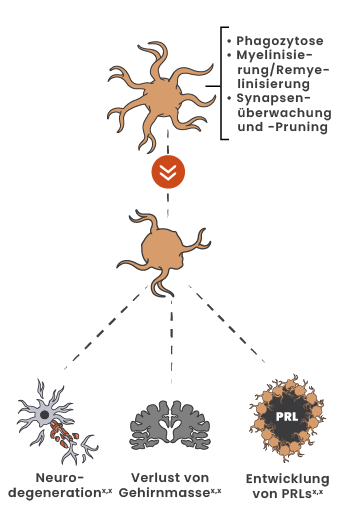
Selbst in frühesten Erkrankungsstadien der MS können Mikroglia von einem homöostatischen in einen krankheitsassoziierten Zustand wechseln21
Krankheitsassoziierte Mikroglia tragen zu axonalem Verlust, Neurodegeneration, Verlust von Gehirnmasse und langfristiger Behinderungsakkumulation bei.22,23

Erfahren Sie es von Expert*innen
Heinz Wiendl, MD, PhD, FEAN, FAAN, erläutert Mikrogila-Aktivierung in der MS auf dem ECTRIMS-Kongress 2023
Mehr entdecken
Die Rolle beider Prozesse verstehen
Referenzen:
-
Giovannoni G, Popescu V, Wuerfel J, et al. Smouldering multiple sclerosis: the ‘real MS’. Ther Adv Neurol Disord. 2022;15:17562864211066751. doi:10.1177/17562864211066751
-
Giovannoni G. The neurodegenerative prodrome in multiple sclerosis. Lancet Neurol. 2017;16(6):413-414.
-
Häusser-Kinzel S, Weber MS. The role of B cells and antibodies in multiple sclerosis, neuromyelitis optica, and related disorders. Front Immunol. 2019;10:201. doi:10.3389/fimmu.2019.00201
-
Krieger SC, Antoine A, Sumowski JF. EDSS 0 is not normal: multiple sclerosis disease burden below the clinical threshold. Mult Scler. 2022;28(14):2299-2303. doi:10.1177/13524585221108297
-
Filippi M, Amato MP, Centonze D, et al. Early use of high-efficacy disease-modifying therapies makes the difference in people with multiple sclerosis: an expert opinion. J Neurol. 2022;269(10):5382-5394.
-
Frisch ES, Pretzsch R, Weber MS. A milestone in multiple sclerosis therapy: monoclonal antibodies against CD20—yet progress continues. Neurotherapeutics. 2021;18(3):1602-1622.
-
Gandhi R, Laroni A, Weiner HL. Role of the innate immune system in the pathogenesis of multiple sclerosis. J Neuroimmunol. 2010;221(1-2):7-14.
-
Reich DS, Lucchinetti CF, Calabresi PA. Multiple sclerosis. N Engl J Med. 2018;378(2):169-180.
-
Hernández-Pedro NY, Espinosa-Ramirez G, de la Cruz VP, Pineda B, Sotelo J. Initial immunopathogenesis of multiple sclerosis: innate immune response. Clin Dev Immunol. 2013;2013:413-465. doi:10.1155/2013/413465
-
Pilz G, Sakic I, Wipfler P, et al. Chemokine CXCL13 in serum, CSF and blood-CSF barrier function: evidence of compartment restriction. Fluids Barriers CNS. 2020;17(1):7. doi:10.1186/s12987-020-0170-5
-
Matejuk A, Ransohoff RM. Crosstalk between astrocytes and microglia: an overview. Front Immunol. 2020;11:1416. doi:10.3389/fimmu.2020.01416
-
Margoni M, Preziosa P, Filippi M, Rocca MA. Anti-CD20 therapies for multiple sclerosis: current status and future perspectives. J Neurol. 2022;269(3):1316-1334.
-
Kamma E, Lasisi W, Libner C, Ng HS, Plemel JR. Central nervous system macrophages in progressive multiple sclerosis: relationship to neurodegeneration and therapeutics. J Neuroinflammation. 2022;19(1):45. doi:10.1186/s12974-022-02408-y
-
Gruber RC, Chretien N, Dufault MR, et al. Central effects of BTK inhibition in neuroinflammation. Presented at: AAN Annual Meeting; April 25-May 1, 2020; Toronto, Canada.
-
Absinta M, Sati P, Masuzzo F, et al. Association of chronic active multiple sclerosis lesions with disability in vivo. JAMA Neurol. 2019;76(12):1474-1483.
-
Friese MA. Widespread synaptic loss in multiple sclerosis. Brain. 2016;139(pt 1):2-4.
-
Jürgens T, Jafari M, Kreutzfeldt M, et al. Reconstruction of single cortical projection neurons reveals primary spine loss in multiple sclerosis. Brain. 2016;139(pt 1):39-46.
-
Werneburg S, Jung J, Kunjamma RB, et al. Targeted complement inhibition at synapses prevents microglial synaptic engulfment and synapse loss in demyelinating disease. Immunity. 2020;52(1):167-182.
-
Keaney J, Gasser J, Gillet G, Scholz D, Kadiu I. Inhibition of Bruton's Tyrosine Kinase modulates microglial phagocytosis: therapeutic implications for Alzheimer's disease. J Neuroimmune Pharmacol. 2019;14(3):448-461.
-
Hendriks RW. Drug discovery: new BTK inhibitor holds promise. Nat Chem Biol. 2011;7(1):4-5.
-
Guerrero BL, Sicotte NL. Microglia in multiple sclerosis: friend or foe? Front Immunol. 2020;11:374. doi:10.3389/fimmu.2020.00374
-
Datta G, Colasanti A, Rabiner EA, et al. Neuroinflammation and its relationship to changes in brain volume and white matter lesions in multiple sclerosis. Brain. 2017;140(11):2927-2938. doi:10.1093/brain/awx228
-
Geladaris A, Häusler D, Weber MS. Microglia: the missing link to decipher and therapeutically control MS progression? Int J Mol Sci. 2021;22(7):3461. doi:10.3390/ijms22073461